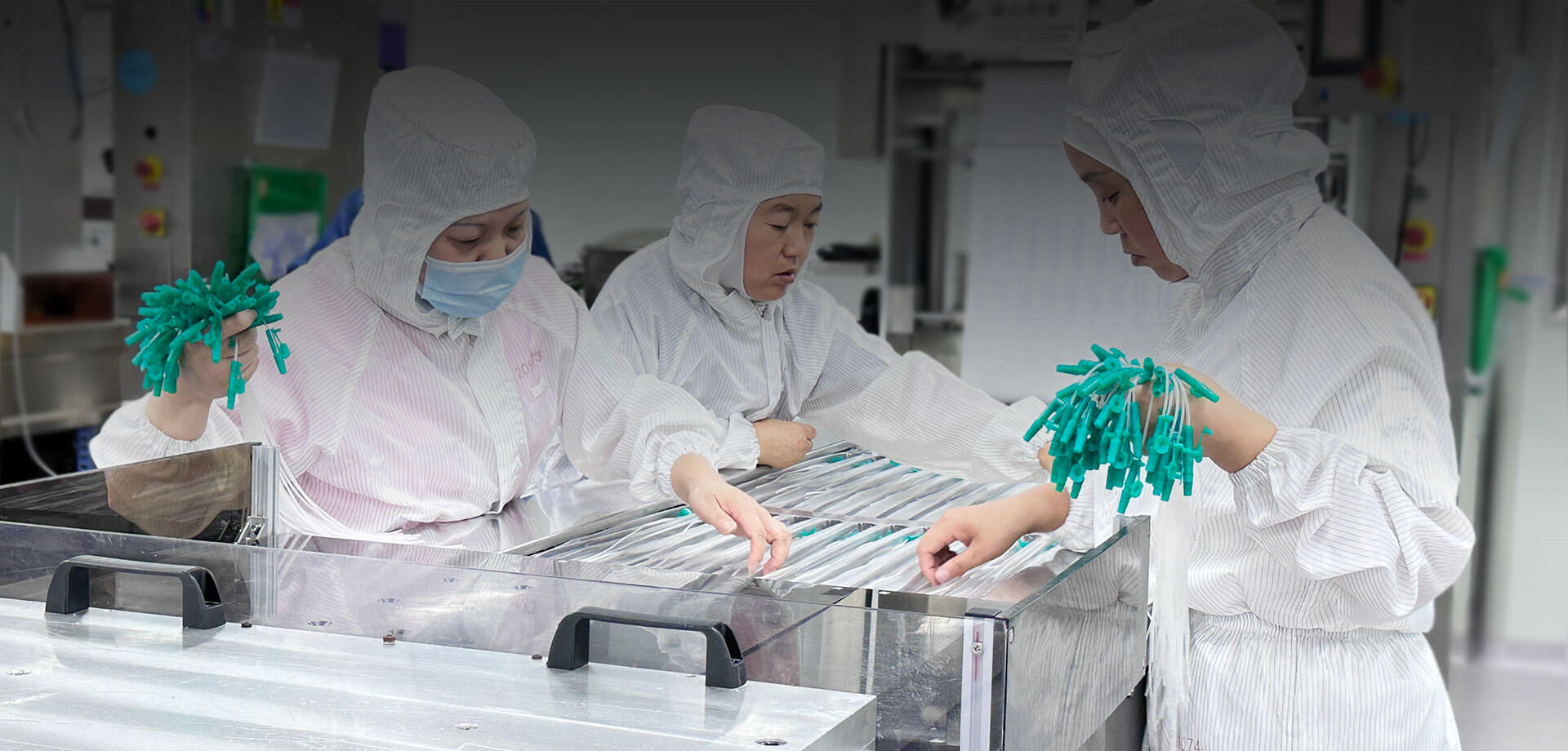
GCMEDICA est un fabricant de fournitures médicales couvrant toute la chaîne industrielle. Fondée en 1998, GCMEDICA se concentre sur la R&D et la fabrication de segments de consommables médicaux et sur l'innovation indépendante de composants de base.
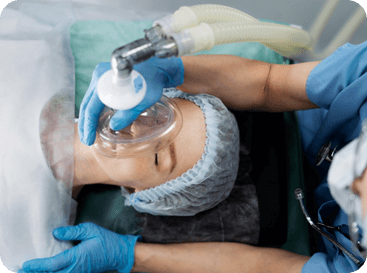
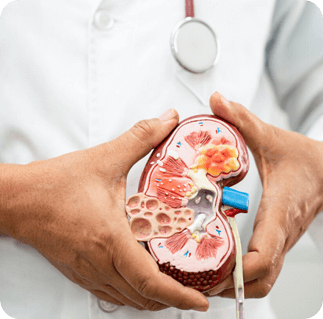
Nos produits comprennent des guides d'intervention mini-invasifs, des cathéters et des consommables pour le bloc opératoire, des consommables pour l'anesthésie et les soins intensifs, ainsi que des consommables respiratoires. Consommables liés aux premiers secours et consommables pour le contrôle et la protection des infections.


 English
English Español
Español